

Results: The use of GnRH agonist in IVF protocols
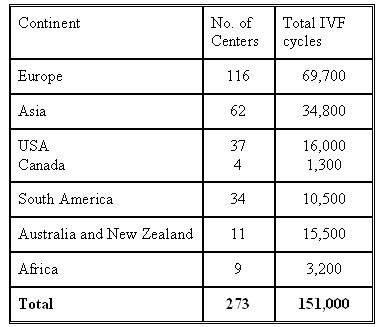
The survey includes reports from 273 centres worldwide performing 151,000 IVF cycles annually.
The survey was compiled by:

Dr. Ilan Tur-Kaspa, Founder and Medical Director, Institute for Human Reproduction (IHR), Professor, Dpet od Ob/gyn, University Chicago, USA.

Prof. Bart Fauser, Head, Department of Obstetrics and Gynecology, University of Utrecht Medical Center, Utrecht, The Netherlands.
 <>
<>
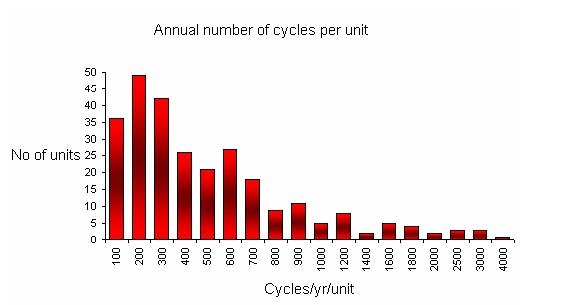
This graph describes the number of cycles performed by each unit participating in the survey. The majority of the units performed up to 400 cycles per year. There was only one unit, reporting to the survey, performing more than 4000 cycles per year.
The use of GnRH agonist
Question 3 in the survey was related the use of GnRH agonists trying to explore the use of this drug in IVF treatment protocols.
Out of 151,000/cycles/y, 134,494 (89.1%) used GnRH agonist.
The use of GnRH antagonist
Question 4 was related to the use of GnRH antagonists and out of 151,000/cycles/y 18,144 (12.0%) were reported using GnRH antagonists.
The above difference is of around 1% showing that the results reported are consistent and probably very accurate.
It can be estimate, on a global scale that around 10%-12% of all IVF cycles are being performed with the use of GnRH antagonists.

Interesting to find is that the 37% used daily injection with decreasing the dose by half when they start stimulation. The use of nasal spay is still very popular. 10% still issue the depot GnRH agonist preparations.
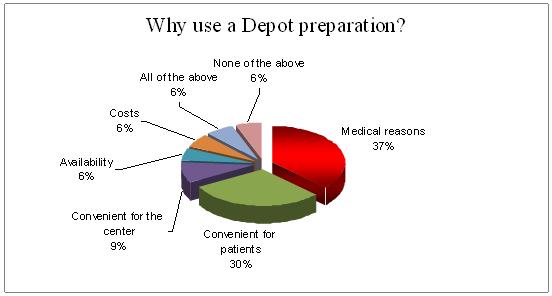
Medical reasons (37%) were the major cause of use of GnRH Depot preparation among the 10% of the cycles in which Depot preparation was used. Second indication (30%) was patient's convenient.
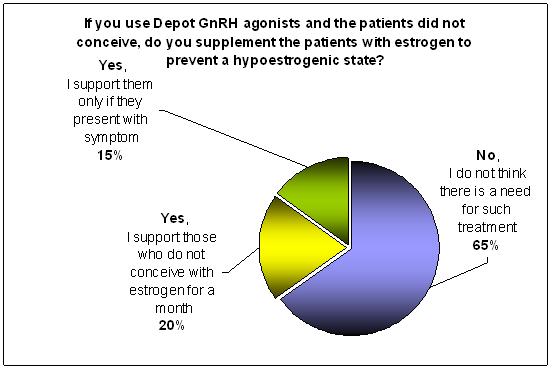
65% of those using GnRH depot preparation do not support their patients with Estrogen if they do not conceived to prevent the unwanted symptoms of chemical induce hypoestrogenic state.
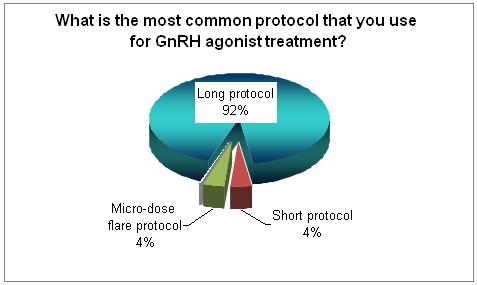
Using the long protocol is still the most popular one.
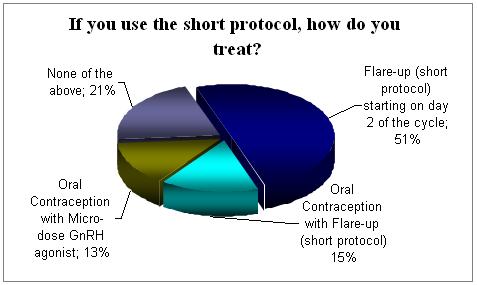
The majority (51%) who used the short protocol start on day 2 of the cycle. There is few other regimens using OC with the agonists.
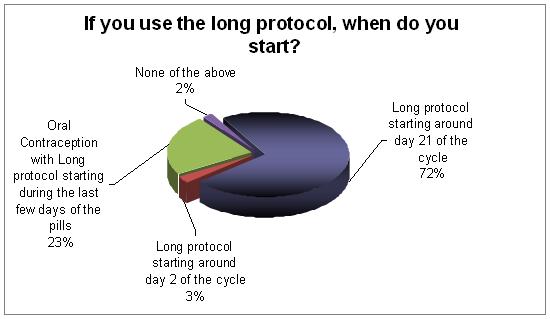
Starting on the mid-luteal phase is now the most common practice. The next common one is starting long protocol during the last few days of the pills.
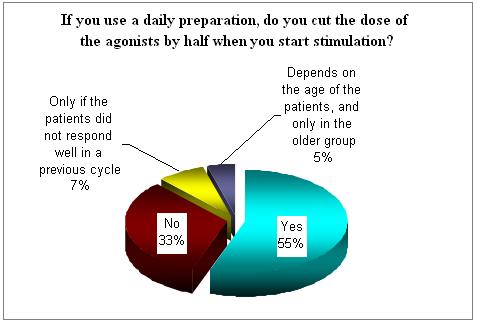
In More than 55% of the treated cycles the agonist dose was cut into half in all patients and in additional 12% if the patients did not responded well. So the majority of the physicians today decrease the dose of the agonist when they start stimulation.
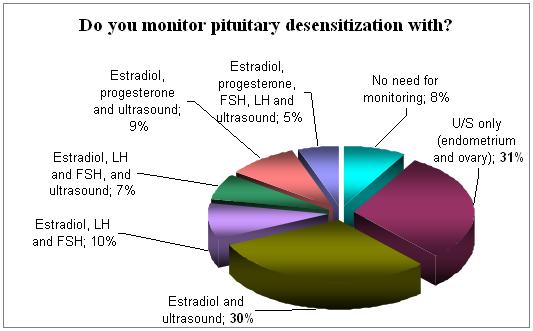
Pituitary desensitization is being monitored in 92% of the survey cycles. Ultrasound is the major tool in this procedure (88%) and serves alone as a monitor in only 30% of the cycles. Ultrasound and serum levels of Estradiol are used in the majority (61%) of cycles for monitoring.
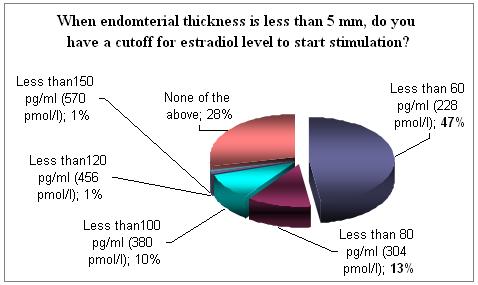
Endometrium thickness serves as part of the monitoring system and this is being done with ultrasound. It seems that those who measure serum Estradiol concentration would estimate this to be below 80-100 pg/ml ( 304-380 pmol).
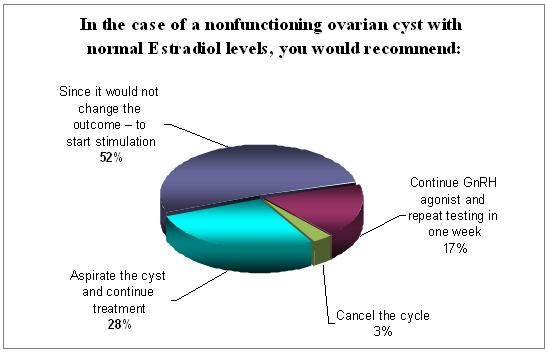
Most of the participants (52%) in the survey believe that the presence of non-functioning ovarian cysts does not influence the outcome and therefore start stimulation. 28% will go forward with the cycle only after aspirating this cyst.
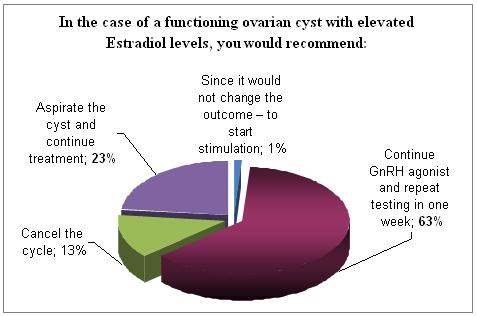
However, in case of functioning cysts, the majority will continue treatment with the agonists. Again 23% (almost similar to the above 28%) will aspirate the cyst. Almost every one agrees that the presence of such a cyst can influence the outcome and 13% will cancel the cycle.
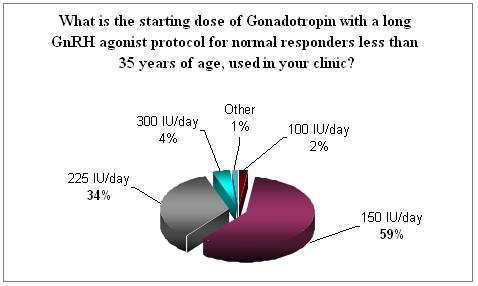
It is a common practice to start treatment with a dose in between 150 to 225 IU of FSH. 59% will start with 150 IU and 34% will start with 225 IU in the young normal responders group. Dosages bellow and above are rare.
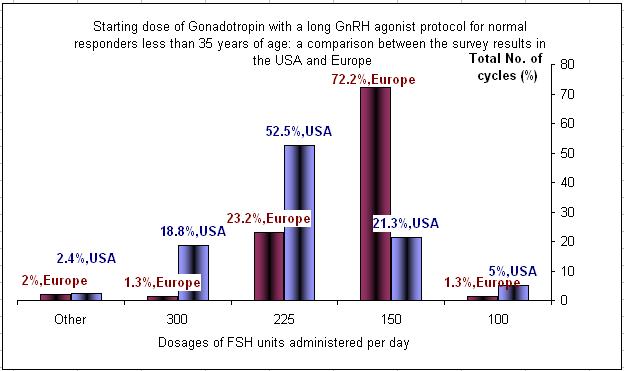
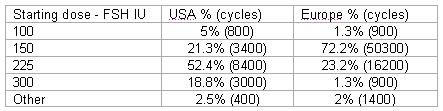
Comparing the above results geographically between the USA and Europe showed major difference in treatment approach. In general the starting dose in the USA is higher for all groups of patients.
<p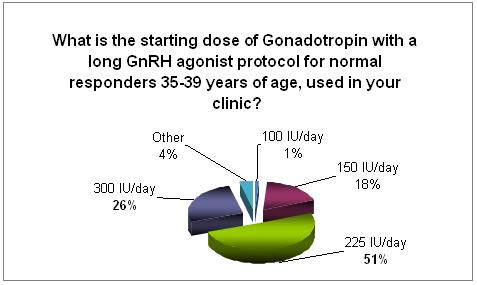
The initial treatment dose of gonadotropin is much higher in the older age group, and it runs in between 225 to 300 IU/d.
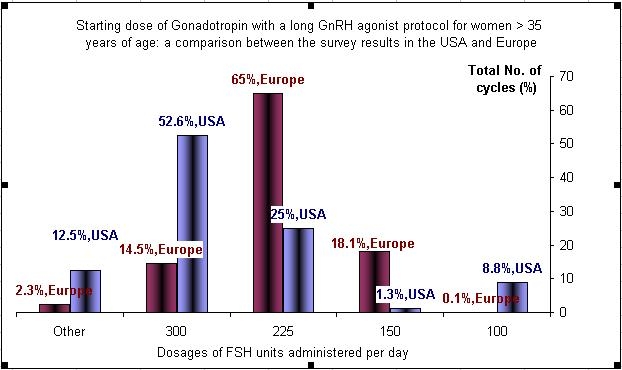
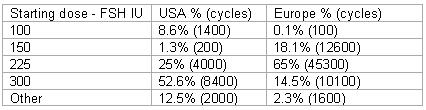
The starting dose of FSH in the USA in most of the cases is higher then the one in Europe.
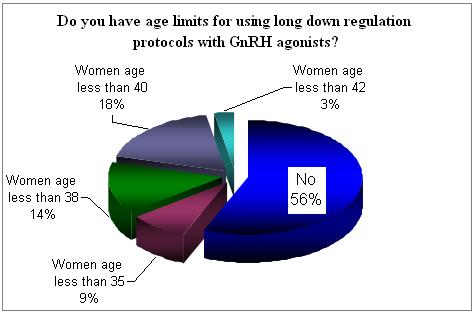
In 56% there is no age limits for the use of long protocol of GnRH agonists. However 44% will eliminate the use of this protocol in the older age group.
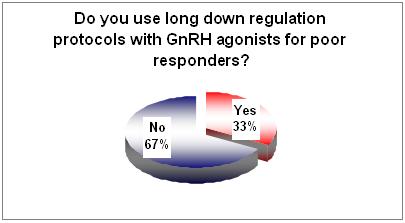
The majority agree that those who define as "poor responders" may benefit from another mode of treatment.
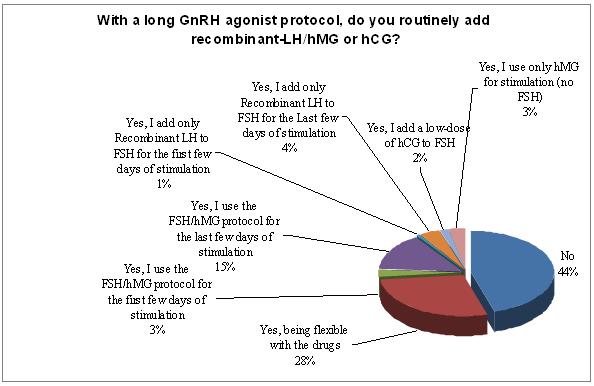
The issue of adding routinely LH is coming back into question. 44% do not add LH as a routine practice and 3% are stimulation with hMG only. 2% are adding hCG as a routine practice. The rest would add either rec-LH or hMG, at the beginning of the cycle or at a late stage of the stimulation but this is only in small percentages. 28% stated that they are flexible both with drugs and the protocols.
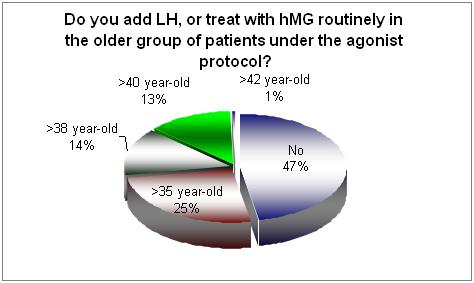
When the issue of adding LH and the older age group was questioned still 47% do not routinely add and sort of LH.
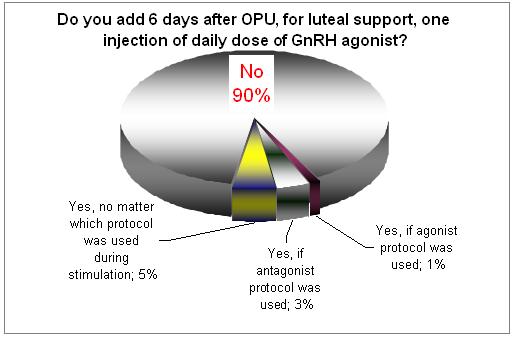
During the last few years several studies recommended the use of GnRH agonist (short acting shot) in the mid-luteal phase. The above results do not confirm that this was accepted in large in clinical practice.
Comments received to the survey:
- Some questions can not be answered for non-agonist users. This practice uses GnRH-agonist as an hCG substitute trigger, however this survey was not intended for this critical information.
- Main use of GnRH agonist is to safely trigger high responders.
- It is worthwhile knowing the agonist preparation one uses as they differ in potency.
- Ultrashort protocol (4 days of GnRH agonist) is a good choice in the first attempt in all groups of patients (low and good responders)
- I do not add routinely LH in the GnRH agonist, but I check the LH level after 6 days of stimulation and I add recombinant LH if the LH is below 1.5 mIU/mL
On behalf of the IVF-Worldwide team Prof. Fauser, Dr. Tur-Kaspa and the Advisory Board of the website, we would like to take this opportunity to thank all the centers that participated in the survey by adding to the global knowledge, as this could be of use around the world.





